By Neil E. Levin
January 2009
One of the strongest examples today of science no longer being self-correcting is the overblown controversy over the safety of vitamin E formulas. This vitamin actually has eight compounds associated with it in the diet: four tocopherols and four tocotrienols. Strictly, vitamin E is only alpha-tocopherol (a-tocopherol; 1 mg = 1.49 IU, international units), whereas these isomers are collectively known as “vitamin E complex.” In 2004, warnings were issued by the authors of a study (Miller et al.) alleging that supplementing 400 IU or more of vitamin E (as α-tocopherol) per day increased the risk of dying of any cause, based on a meta-analysis of results collected from 19 individual studies. Only one of these studies utilized high-potency vitamin E and had a large population (20,536), though reporting “no significant differences in all-cause mortality” (MRC/BHF Heart Protection Study). Combining inconsistent forms/doses of the vitamin introduced additional variables, while positive effects of the vitamin were ignored. The exclusion from the meta-analysis of a dozen otherwise eligible studies in which fewer than 10 patients died created controversy over its methodology. Miller et al. acknowledged, “We could not evaluate the generalizability of our findings to healthy adult populations.”
Leading antioxidant researchers collaboratively reviewed the individual datasets and published their results in the American Journal of Clinical Nutrition (Hathcock et al.), reporting that daily doses of α-tocopherol up to 1,600 IU are generally safe. In fact, Hathcock et al. stated that, after properly adjusting for variables in supplementation, the dose of vitamin E that may have been harmful to seriously ill patients in the Miller et al. report was statistically significant only at levels over 2,000 IU per day, well above the 400 IU estimated in that original report.
Similarly, the US Institute of Medicine set the safe upper level of vitamin E at 1,500 IU daily. And the SENECA study (Survey in Europe on Nutrition and the Elderly, a Concerted Action) of 90,000 nurses showed a 30-40% lower incidence of heart disease among those with the highest intake of vitamin E from diet and supplements (Stampfer et al.). Clearly, the report by Miller et al., which is still being cited by most vitamin E studies, is unrepresentative of the body of science and was not successfully replicated by Hathcock et al. But inexpert meta-analyses can multiply variables; in this case, some studies were arbitrarily excluded while key factors such as diet and antioxidant synergies were ignored. The fact that Hathcock et al. reanalyzed the data and reached quite different results is telling. Yet that authoritative report has been virtually ignored by the scientific and media communities, who still constantly repeat the Miller group’s allegation that vitamin E is unsafe.
Mistaking statistics for scientific fact
The straight mathematical integration of data from different selected scientific studies in the Miller et al. work-and the interpretation of the results-were heavily criticized in subsequent comments appearing in the Annals of Internal Medicine. Consequently, the reputation of most vitamin E complex products among consumers continues to reflect that negativity.
Media mistake:
Making a mountain out of a molehill
The popular press presented the outcome of the Miller group’s study as being more meaningful than it really was, using one analysis to negate many studies and virtually ignoring the reanalysis. To this day, journalists (and researchers!) cite only the Miller et al. report-even though vitamin E has been repeatedly proven safe and beneficial in more robust studies.
Vitamin E: A tale of two studies
Two large studies, both published in the same issue of the refereed journal Cancer Epidemiology, Biomarkers, & Prevention, have reached contradictory results as to how supplemental vitamin E affects prostate cancer. But are both equally meaningful? Actually, one is far more rigorous than the other.
In the first study (Wright et al.), only food sources containing a-tocopherol were effective at reducing prostate cancer risk, but not supplemental vitamin E as a-tocopherol. This study looked at questionnaires related to subjects’ intake of vitamin E from food and supplements at the start of the study, then compared the number of cancers over a five-year period with data obtained from that questionnaire.
In the second study (Weinstein et al.), definite large benefits were shown for supplemental a-tocopherol vitamin E, but not for food sources containing mostly γ-tocopherol (the gamma form). A closer look reveals that this study looked at serum levels along with food and supplemental vitamin E intake and then related that data to prostate cancer rates up to 19 years afterward. This study concluded: “In summary, higher prediagnostic serum concentrations of α-tocopherol, but not dietary vitamin E, was [sic] associated with lower risk of developing prostate cancer, particularly advanced prostate cancer.”
The measurement of serum levels in the body, along with careful reporting of a nutrient’s intake from various sources and other synergists, is far more compelling than a questionnaire completed by notoriously faulty human memory, then assuming that the answers were accurate or relevant five years later. A cancer study lasting nearly four times as long is more compelling than a shorter one because it is more likely to encompass the cancer’s incubation period and allow for the development of symptoms that allow detection. As the National Cancer Institute reports: “Prostate cancer often does not cause symptoms for many years.”
Reputable studies support the use of supplemental α-tocopherol to enhance human health. The Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study demonstrated a 32% reduction in prostate cancer incidence in response to daily a-tocopherol supplementation. Vitamin E consumption levels above 100 IU daily are associated with decreased risks of coronary heart disease and certain types of cancer. Intakes considerably above levels obtainable from diet result in enhanced immune function as well (Weber et al.).
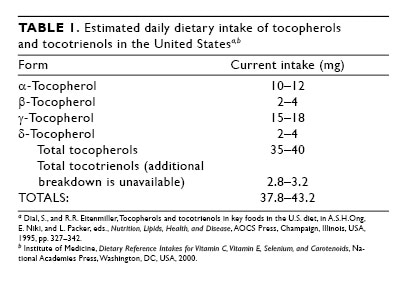
The typical daily intake of a US resident (Table 1) is well below the Recommended Daily Allowance of 22.5 IU, equal to 15 mg (Ervin et al.).
Commentary
There is a general need for supplemental vitamin E complex, unless we all suddenly decide to eat wholesome natural foods containing a lot more vitamin E-a desirable but unlikely outcome. Nor do studies typically measure synergistic antioxidants, including the tocotrienols, that affect vitamin E status. Since the γ- and d-tocopherols and tocotrienols are better antioxidants than the α forms, they can better maintain serum levels of α-tocopherol in its reduced form. If these studies were put into proper perspective, we could accurately assess their value. Unfortunately, media coverage of negative reports, especially regarding vitamins, drowns out the positive ones, even when the good news is from more rigorous studies. The low amounts of vitamin E in current US diets should be increased to provide adequate mixed tocopherols and tocotrienols.
Neil E. Levin is a board-certified clinical nutritionist with a Diplomate in advanced nutritional laboratory assessment. He is the nutrition education manager and a product formulator for NOW Foods, a natural food and dietary supplement manufacturer headquartered in Bloomingdale, Illinois, USA. He blogs at www.honestnutrition.com and can be contacted by e-mail at neil.levin@nowfoods.com .