IOM panel recommends tripling vitamin D intake: Panel’s conservative approach receives criticism
By David Piller
September 2011
The following article is based on the Hot Topic Symposium, “Vitamin D: New Dietary Intake Recommendations and Emerging Health Effects,” and subsequent panel discussion, which took place during the 102nd AOCS Annual Meeting & Expo, held in Cincinnati, Ohio, USA, May 1–4, 2011. The vitamin D panel discussion and video clips can be found at the AOCS Vitamin D resource page: http://tinyurl.com/AOCSmultimedia.
In November 2010, the Food and Nutrition Board of the US Institute of Medicine (IOM) recommended that daily vitamin D consumption should be tripled from a level of 200 International Units (IU) to 600 IU for most adults up to age 70. Although the new recommendation is welcome news for a large portion of the medical community, it still fails to meet the expectations of many who are calling for still higher recommended levels.
In recent years, vitamin D has been touted as a panacea of sorts, with reports claiming its benefits in reducing all manner of chronic conditions from memory loss to cancer. With such a wide range of information being disseminated on vitamin D, the US and Canadian governments requested that the IOM form a panel to revise recommendations on vitamin D intake that have been in effect since 1997. Vitamin D is naturally present in very few foods; rather, vitamin D is produced in skin cells exposed to ultraviolet radiation from the sun. It is added to some foods, though, and is very popular as a dietary supplement.
The IOM panel consisted of 14 scientists who met eight times to review more than 1,000 studies that have been published on the health effects of vitamin D. While it has long been established that vitamin D is essential to maintaining bone strength, many published studies have also linked low vitamin
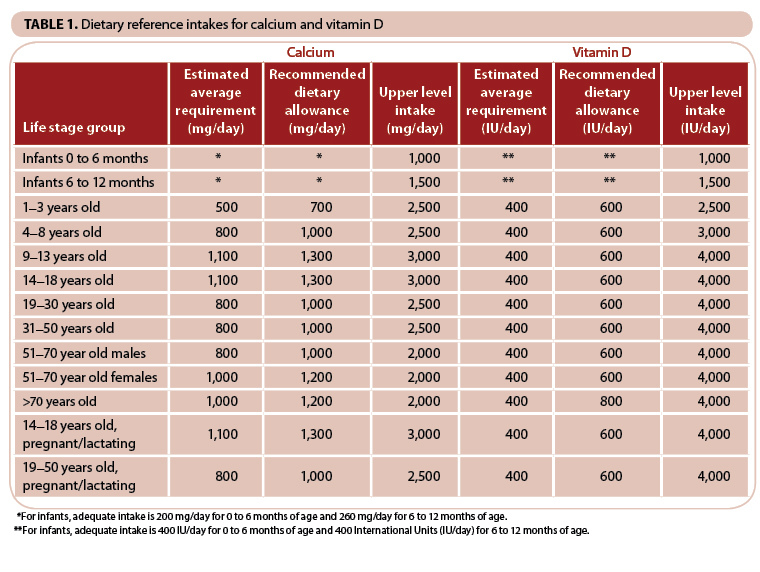
D levels to an increased risk of health problems ranging from heart disease and cancer to depression and cognitive decline. The IOM panel, however, did not find sufficient evidence that vitamin D provided further health benefits, concluding that most published health benefits associated with vitamin D provide “mixed and inconclusive results and could not be considered reliable.” The panel therefore based its new recommendations (Table 1) solely on vitamin D levels needed to maintain strong bones.
{kind=link}
There have long been concerns that many people have vitamin D levels that are considered deficient. The panel, however, concluded that 97.5% of the population has blood serum concentrations of 25-hydroxy vitamin D above 20 nanograms per milliliter (ng/mL), a level it says is sufficient for bone health.
The new recommendations, which cover the United States and Canada, call for intakes of 600 IU daily for children age 12 months and above through adults age 70 and 800 IU after age 71. The previous adequate intake recommendations were 200 IU per day for infants through age 50, 400 IU per day for ages 51 to 70, and 600 IU per day for those 71 and older. The panel also raised the acceptable upper limit of daily intake to 4,000 IU for adults, from 2,000 previously.
A cautious approach
The recommendations, while earning praise as a step in the right direction, have generated a fair amount of criticism from medical practitioners and organizations for not going far enough. Patsy Brannon, a member of the IOM panel, counters that it was incumbent upon the IOM committee to take a very cautious approach. Brannon, a professor in the division of nutritional sciences at Cornell University (Ithaca, New York, USA), says the evidence from the myriad studies the panel considered simply was not robust enough to make more dramatic recommendations. Even when it came to the one factor where the evidence of a direct link to vitamin D was most compelling—bone health—Brannon says most studies have been done looking at causal effects of vitamin D and not dose response. In addition, most studies examine only one dose, so determining an optimal dosage became a difficult task. “It is a challenge, and it involves scientific judgment,” she says. “One of the charges for us in the report was to be clear about what the limits of the evidence were, where the gaps were, and how we were making our decisions based on our judgment.”
To determine how much vitamin D is needed, Brannon says the panel first had to determine what level of serum 25-hydroxy vitamin D was necessary to maintain bone health. “The committee had to link bone health outcomes with serum 25-hydroxyvitamin D levels because the limitations in the evidence don’t allow us to look just at vitamin D intake per se,” she explains. “We looked very carefully at outcomes related to skeletal health and we linked 20 ng/mL of 25-hydroxy vitamin D with skeletal health. That was very helpful in helping us determine how much vitamin D you need to consume in order to achieve that level of serum 25-hydroxy vitamin D.”
For some practicing physicians, the panel’s recommendations are not consistent with the anecdotal evidence from their day-to-day practice. They have seen literature that links deficient vitamin D levels to an increased risk for diseases, including cardiovascular disease, certain types of cancer, autoimmune disease, and many more. In addition, they have observed markedly improved outcomes in their own practice when they test for and prescribe higher levels of vitamin D. Many physicians, in fact, have begun testing their patients’ 25-hydroxy vitamin D serum levels as part of their routine physicals.
Steven Clinton, a professor in the Division of Medical Oncology at The Ohio State University (Columbus, USA) and a member of the report’s review committee, says the findings in the report do not back up extensive testing. “This committee would not recommend that a vitamin D workup be part of a healthy clinical visit,” says Clinton. “On the other hand, if someone is seeing a physician with an illness or a symptom that could be related to vitamin D, that is when it’s appropriate to be checking for vitamin D levels.”
Clinton points to the committee’s recommendation that national standards for vitamin D tests be established. Along with standard tests, the report also calls for agreed-upon normal ranges of serum 25-hydroxy vitamin D based upon the latest scientific evidence.
There remains, though, a large disparity between the anecdotal evidence from the doctor’s office and the recommendations of the panel. Many physicians were highly critical of the 600 IU level, saying it should instead be closer to 2,000 IU. Gregory A. Plotnikoff of the Allina Center for Health Care Innovation at Abbott Northwestern Hospital (Minneapolis, Minnesota, USA) sums up the difficulty faced by the IOM panel. Plotnikoff, who is an advocate of much higher levels, sees firsthand the markedly improved outcomes for his patients who suffer from conditions such as chronic pain when he measures for and replenishes vitamin D levels. He also understands, however, that his diagnosis and treatment are not based on hard clinical evidence, but rather on his own clinical judgment. “If we measure (vitamin D levels) and they’re low, and we replenish to some given level, does that make a clinical difference? There’s a huge missing research component in that regard,” he says. “What I need as a physician is very different from what we as a society need for a public health recommendation. And that’s where the struggle around the report has come. The mandate of this committee was to be cautious because these are long-lasting recommendations.”
The need for further clinical research to determine vitamin D’s benefits in conditions beyond bone health is clear. “I would hope that we would have more and well-designed randomized clinical trials to help us know whether there is a causal role with vitamin D and all these intriguing linkages with so many chronic diseases,” says Brannon. “And I would hope that we would have some sort of fundamental basic science that would help us understand some real key points about vitamin D metabolism.”
More evidence is coming
One such study is now under way. The US National Institutes of Health is funding a $20 million study to determine whether vitamin D has benefits other than bone health. The five-year randomized trial, which began in January 2010, is currently recruiting 20,000 men and women over age 60. The aim of the study is to determine whether taking 2,000 IU of vitamin D or marine omega-3 fatty acid (eicosapentaenoic acid + docosahexaenoic acid) supplements reduces the risk for developing cancer, heart disease, and stroke in people who do not have a prior history of these illnesses.
This study and others looking at specific disease states will go a long way in determining whether vitamin D continues to be known as an effective treatment for a host of chronic, and often deadly, diseases. Even the IOM panel members believe there is a distinct possibility it will be proven to be as good as advertised. It is just going to take a little longer for the rigorous science to catch up.
David Piller is a freelance science and health writer based in Cincinnati, Ohio, USA. A professional writer for more than 20 years, he has produced feature articles, web content, marketing communications, and technical documentation for both public and private healthcare organizations.
Was Mozart vitamin D-deficient?
The cause of the early death at age 35 of composer Wolfgang Amadeus Mozart has been a source of conjecture for more than 200 years. Among the possibilities are poisoning, infection, cardiovascular disease, and renal disease and its complications.
A letter in the journal Medical Problems of Performing Artists (26:117, 2011) suggests that vitamin D deficiency may have played a role in the many illnesses Mozart suffered during his lifetime as well as his early death. Authors William B. Grant and Stefan Pilz note that he composed mainly at night and so would have slept during the day, causing reduced sunlight-induced vitamin D synthesis. Further, they write: “Mozart died on December 5, 1791, two to three months into the vitamin D winter [in Vienna]. The half-life of 25(OH)D [25-hydroxy vitamin D] in the human body is four to six weeks; his serum 25(OH)D levels would have been very low.”
Vitamin D and cancer: much hype, some hope
In what seems like a nearly daily occurrence, research studies finding more and better benefits of vitamin D are being reported in the media. Vitamin D’s role in fighting cancer is prominent among these. Studies have reported risk reductions for a range of cancers, including colorectal, breast, oral, stomach, and pancreatic.
With so much information coming out, Steven Clinton says, there is a need to analyze the information from the perspective of hard science. Clinton, along with JoAnn Manson from Harvard and Susan Mayne of Yale, did just that in a recent report published in the New England Journal of Medicine (364:1385–1387, 2011).
The authors acknowledged in the commentary that the enthusiasm generated by these studies is warranted by the “biological plausibility” that vitamin D can reduce the risk of cancer. But the authors, who participated in the exhaustive literature review on the IOM panel, said evidence that vitamin D reduces cancer incidence was inconsistent and inconclusive. In addition, they said, the evidence does not establish a cause-effect relationship.
The problem, according to the authors, is that, to date, there have been no large randomized clinical trials that associated vitamin D with cancer specifically. Most of the current evidence has been derived from laboratory studies, ecological correlations, and observational investigations.
“New trials assessing moderate- to high-dose vitamin D supplementation for cancer prevention are in progress and should provide additional information within five to six years,” the authors conclude. “Although future research may demonstrate clear benefits of vitamin D related to cancer and other nonskeletal health outcomes, and possibly support higher intake requirements, the existing evidence falls short.”
Vitamin D 101
The term vitamin D actually refers to a group of several very closely related fat-soluble compounds that are structurally similar to sterols but function like hormones. In plants, vitamin D is present in the form of ergocalciferol (vitamin D2). In animals, it is present in the form of cholecalciferol (vitamin D3).
According to the University of California at Riverside’s Vitamin D homepage (http://vitamind.ucr.edu/chem.html), vitamin D is derived from a steroid, so the structure retains the numbering of its parent compound, cholesterol. Asymmetric centers are designated by using the R,S notation; the configuration of the double bonds are notated E for the German “entgegen” or trans, and Z for “zuzammen” or cis. Thus, the official name of vitamin D3 is 9,10-seco(5Z,7E)-5,7,10(19)cholestatriene-3b-ol, and the official name of vitamin D2 is 9,10-seco(5Z,7E)-5,7,10(19), 22-ergostatetraene-3b-ol.
Vitamin D3 is produced photochemically when ultraviolet (UV) light from the sun activates a precursor sterol (7-dehydrocholesterol), which is present in the epidermis of most animals. A conjugated double bond system in the B ring of this sterol allows the absorption of light quanta at certain wavelengths in the ultraviolet (UV) range, which initiates a complex series of transformations that ultimately result in vitamin D3. Vitamin D3 is then absorbed in the small intestine, where it binds to plasma alpha 2 globulin and enters the bloodstream. It is then transported to the liver, where it is turned into calcidol [25-hydroxy vitamin D]. Calcidol, in turn, is transported to the kidneys and transformed into the steroid calcitriol, which is excreted into the blood to help regulate calcium in the body.
Meanwhile, tissues other than the kidneys turn calcidiol into calcitriol to help regulate gene expression locally—both inside the cell (autocrine) and surrounding the cell (paracrine). The use of calcitriol by other tissues as an autocrine and paracrine hormone is a relatively new discovery that explains its role in human development as well as its benefits in other illnesses such as diabetes, hypertension, heart disease, autoimmune illnesses, cancer, and, perhaps, mental illness.
According to John Jacob Cannell, executive director of The Vitamin D Council (San Luis Obispo, California, USA), young adult Caucasians produce about 20,000 international units (IU) of vitamin D in their skin within minutes of whole-body, summer sun exposure (see http://faculty.irsc.edu/faculty/jschwartz/Vit D.htm). In other words, light skinned individuals could greatly exceed the IOM’s vitamin D intake recommendations simply by spending a few minutes outside in their swim suits. Vitamin D3 can also be obtained by eating certain animal foods, such as mackerel, cod, salmon, shrimp, eggs, butter, beef, and chicken livers. Vitamin D2, which is equivalently potent to vitamin D3 in humans and many mammals, but not in birds, is produced naturally by mushrooms and commercially by the irradiation of the plant sterol ergosterol with UV light.
“We are all waiting for the 900 or so randomized controlled trials that scientists are conducting using vitamin D,” Cannell noted in a news release discussing the outcome of one of the first such, albeit small (44 subjects), trials. The study was published in the American Journal of Clinical Nutrition (doi:10.3945/ajcn.111.011684).
A research team led by Anastassios Pittas of Tufts Medical Center in Boston, Massachusetts, USA, reported that 2,000 IU/day of vitamin D, given for 12 weeks, significantly improved pancreatic function in mildly overweight adults with prediabetes. Cannell took issue with the “low dose” administered in the study—the Vitamin D Council recommends a daily intake of 5,000 IU—noting that the study intake level “only increased vitamin D levels from 24 to 30 ng/mL.” Pancreatic function, however, as measured by changes in the subjects’ disposition index, increased by 300 in the vitamin D group but fell by 126 in the placebo group. (Disposition index is a quantitative measure that describes the relationship between β-cell sensitivity and insulin sensitivity.)
“I predict that after most of the randomized controlled trials are out—in another 10 years—the Food and Nutrition Board [of the US Institute of Medicine] will meet again and say, ‘Whoops, it should have been 5,000 IU/day all along,’” Cannell wrote.
The calcium and Vitamin D link
The IOM recommendations not only include new levels for vitamin D, they also provide new recommendations for daily calcium intake. Some of the highlights include:
- 700 milligrams (mg) for children aged 1 to 3
- 1,200 mg for women 51 and older
- 1,000 mg for men 50 to 70
The panel also noted that teenage girls may not get enough calcium, and that postmenopausal women may get too much, running the risk of kidney stones.
Though the new calcium levels are not receiving the attention (or controversy) of the vitamin D recommendations, the two are inextricably linked. “Calcium is absorbed through two pathways; one that requires vitamin D and one that doesn’t,” says Connie Weaver, professor and head of the Department of Foods and Nutrition at Purdue University (West Lafayette, Indiana, USA). “You need quite a bit of calcium to only use the pathway that doesn’t require vitamin D, and that’s beyond what most people take.”
An adequate supply of vitamin D is necessary to best utilize calcium. “Calcium and vitamin D are very intimately linked because calcium is a major constituent of bone,” says Weaver. “You need to have it absorbed from the diet and transferred to the bone.” And, because the body cannot get calcium from a source other than diet or supplements, Weaver says it’s vital that people get the recommended amount of calcium, especially in their early years.